
What is a Circumferential Abdominoplasty?
This is the ultimate re-contouring procedure for the trunk. It addresses everything the extended abdominoplasty does, with the addition of excising excess lower back skin and elevating the buttocks.
When is a Circumferential Abdominoplasty necessary?
The most common reason to perform this procedure is massive weight loss such as following bariatric surgery for morbid obesity or after dietary weight loss of 70 seventy pounds or more, and more often over one hundred pounds. While pregnancy usually results in stretching of the trunk contours in the front only, morbid obesity is a circumferential disease process that causes stretching of the skin completely around the trunk with sagging of the lateral thighs, buttocks, and excess skin of the hips, flanks and lower back. When this is the case, any procedure less than this is really not going to do a good job of re-contouring the trunk.
What is the Circumferential Abdominoplasty procedure?
The procedure is performed in a way similar to the extended abdominoplasty except that when the patient is placed on their side, the incisions are carried all the way to the midline of the back, just above the upper portion of the gluteal cleft (the vertical space between the buttocks). I prefer to perform this procedure a little differently. First, the patient is operated while lying on their stomach, and then turned onto their back. It is an extremely powerful procedure and the results after surgery are often so drastic that its hard to believe the before and after appearances are really the same person! Depending upon the patients underlying medical conditions and the amount of tissue to be removed, I sometimes prefer to keep the patient overnight for observation in the hospital. In other patients, I perform this surgery in my office-based surgical facility.
Step 1
Click to Enlarge
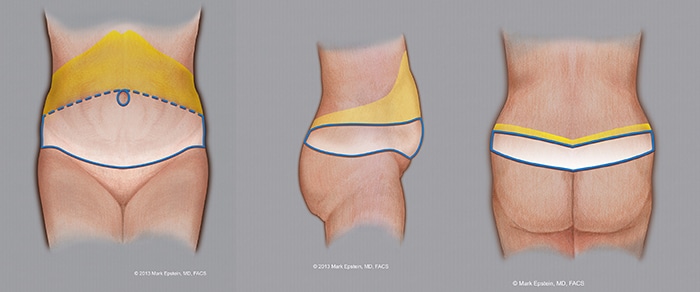
The blue ellipse indicates the proposed amount of skin to be removed. The lower solid blue line is where the initial incision is made. The dotted blue line is the proposed upper portion of the skin excision (removal). This can vary upwards or downwards depending upon how much skin excess exists. The blue circle around the navel (umbilicus) represents the incision around the umbilicus. The umbilicus remains attached to the underlying abdominal muscles and is not lifted upwards with the remaining abdominal skin. This leaves a circular hole in the skin flap (see Step 5). The yellow area shows the extent to which the abdominal skin is elevated off the abdominal wall. The incision ultimately extends to the posterior flanks all the way to the midline. This procedure is performed with the patient first on their back, then after the front has been completed, the patient is turned on their right side, then onto the left side (or start with patient on their stomach, then turn patient onto their back).
Step 2
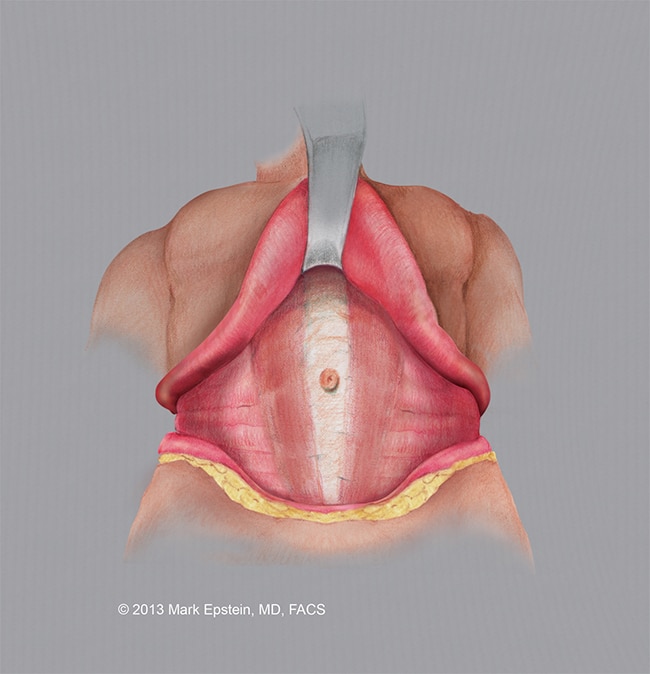
The abdominal skin is elevated off the abdominal wall, the abdominal musculature is revealed. Note, the umbilicus remains attached to the muscle in the midline. The area of surgical dissection extends to the flanks, further than during a standard abdominoplasty.
Click to Enlarge
Step 3
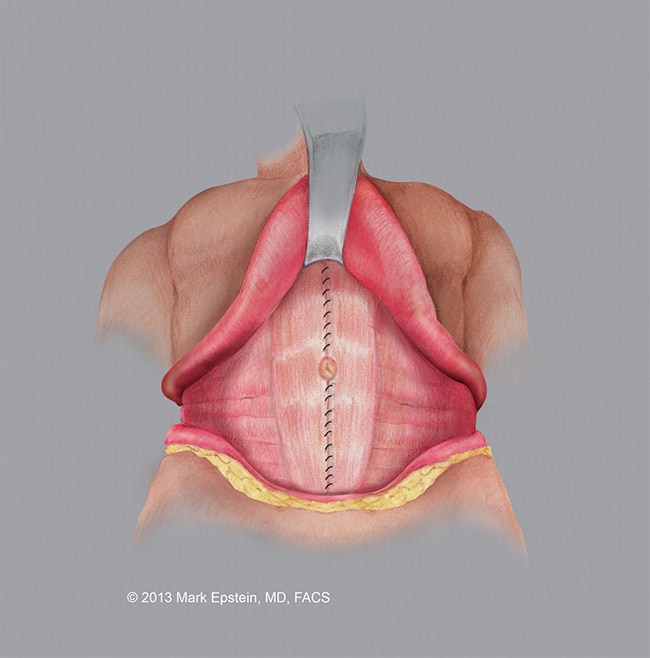
The abdominal wall musculature is tightened using a special running suture. The muscles are brought together in the midline.

Click to Enlarge
Step 4
The completed repair of the abdominal musculature is shown.
Click to Enlarge
Step 5
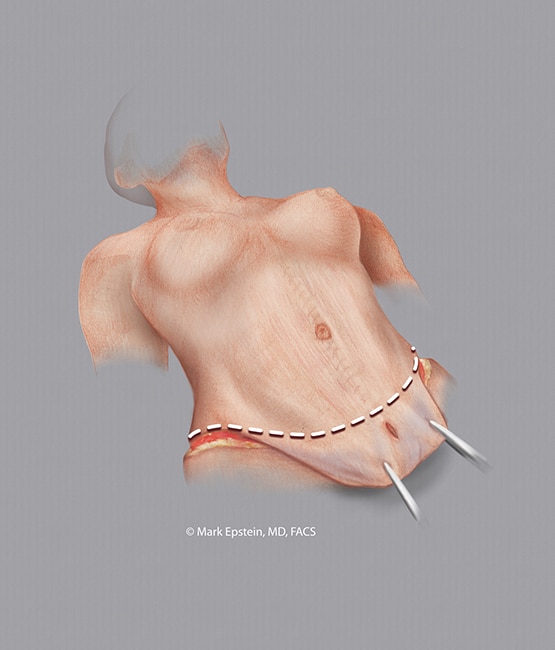
The excess skin is elevated above the abdominal wall and pulled downward. The area of resection (removal) is indicated with a dotted line. The original hole in the abdominal skin is below the line of resection (removal of skin) and therefore is removed with the abdominal skin.
Click to Enlarge
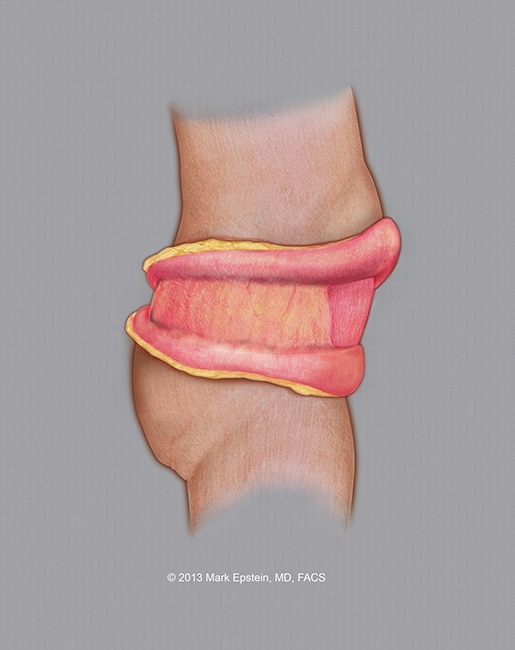
Step 6
The flank wound exposed. The skin is elevated above and below, the excess is trimmed and then the wound is closed. There is no need to tighten the musculature. This portion of the procedure is usually performed after the front of the abdomen has been completed and the wound closed. The patient is turned onto one side, then the procedure is repeated on the other side. This is because it is often impossible to access the posterior flank when the patient is lying supine (on their back). In the alternative, the flanks and back can be addressed at the beginning of the procedure with the patient lying prone (on their stomach), after this is completed, the patient is then placed on their back and the front is completed. This is my preference.
Click to Enlarge
Step 7

Click to Enlarge
Click to Enlarge
The final result of the front portion of the procedure is shown on the left with the location of the scar across the waist crease of the abdomen as well as a scar around the umbilicus. After this portion is completed, the wound is dressed and the patient is turned onto their right side for excision of excess flank skin.
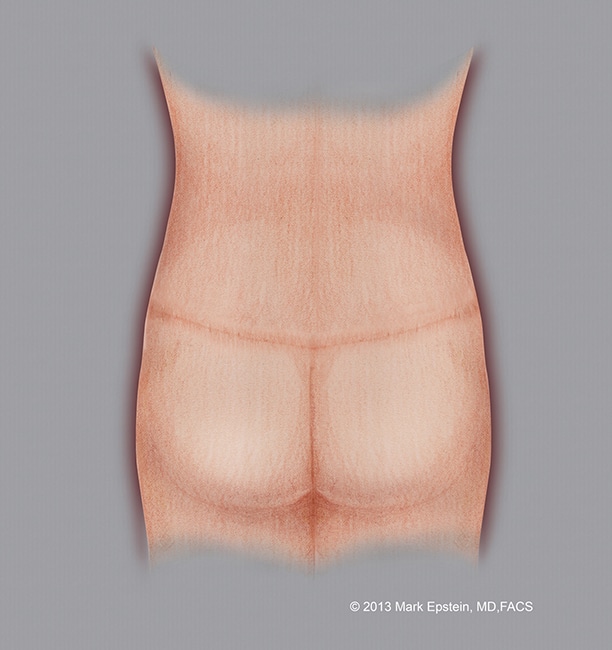
Lastly, the procedure is repeated on the left side. In the alternative, the patient can be placed prone (on their stomach) and undergo excision of both sides of the back and flanks simultaneously, then turned onto their back for the front portion of the procedure. The final closure of the back is shown on the right.
Schedule A Consultation
To learn more about our Circumferential Abdominoplasty procedures, please call us at 631.689.1100 to schedule a consultation with Dr. Epstein. Our practice is proud to serve Haupaugge and the surrounding areas of Long Island, NY.
Sections - Abdominoplasty Types
- Why Do We Need Different Types Of Abdominoplasty?
- Standard Abdominoplasty With “Umbilical Re-Positioning”
- Standard Abdominoplasty with a “Floated Umbilicus”
- Mini-Abdominoplasty
- Extended Abdominoplasty
- Circumferential Abdominoplasty “Belt-lipectomy”
- Flowchart – How to Select an Abdominoplasty Procedure
Prev Chapter: How is an Abdominoplasty Performed? »
Next Chapter: Combination VASER/PAL HI-Definition Lipo-Abdominoplasty »
