
Just like in the case of lower pole stretch/inferior implant malposition, lateral displacement/implant malposition represents a spectrum of two separate deformities as well. All breast implants cause lateral stretch. From an aesthetic standpoint, the lateral part of the breast needs to stretch to give roundness to the breast and “lateral protrusion” – where the outer edge of the breast lies beyond the outer border of the chest wall to balance the hips and give rise to the hourglass curve of the female form. If you look at a woman right after breast augmentation, the outer breast looks flat and tight, just like the bottom of the breast. In order to achieve a proper aesthetic result, we are depending on the breast tissue to stretch. The art and skill of breast augmentation is assessing a woman’s breast dimensions and tissue quality, then knowing how to make the implant pocket, select the right size and shape implant such that when all is said and done, and the breast has healed and settled, the curvature of the breast looks as perfect as possible, every time you perform this surgery! Talk about pressure!!!
The issue here is that in some women, when they are standing upright the breasts are right where they should be, but when they lie down, the breasts move to the sides of the chest and they lose their medial (inner breast) fullness. Why does this happen? Well, just like with lower pole stretch/inferior implant malposition, this happens to some degree a fair amount of the time but the aesthetics of the breast are not compromised. The problem is when it becomes excessive, it catches the attention of the patient. As a surgeon does not routinely examine patients after breast augmentation flat on the table, the surgeon is not the one to pick this up. It is the patient who brings it to her surgeon’s attention. Then a simple examination in the supine (on your back) position will confirm the problem. So why does this happen?
When the implant pocket is created, just as the lower portion of the pocket is defined as the lower breast crease, there is also a lateral (outer) breast border that must be defined. If you do not set the lateral edge of the pocket far enough laterally towards the outer chest, the breast will look pushed inwards towards the breastbone with a flattened outer contour. If you set the border too far towards the back, the implants (and the breasts) will lie too far apart. This is usually noticeable early on after surgery. Most surgeons create the pocket using blunt dissection – essentially pulling and tearing the muscle and breast tissue away from the chest wall as well as from each other. This leads to lack of control of implant pocket dimensions and certainly, it is possible when the pocket is dissected too far laterally the implants may fall to the sides when this occurs. If this is recognized at surgery, although best if it didn’t happen in the first place, the outer edges of the pocket can be sewn back down to the chest wall in an attempt to correct this. When this is done later when a scar tissue capsule is now lining the pocket, it is called a lateral capsulorraphy. When I create the implant pocket, I do so using precise electrocautery dissection, a technique where absolutely no blunt dissection is performed. There is a dramatic reduction in both blood loss and pain, and much greater control over the dimensions of the pocket. In my practice, I do not see laterally over-dissected pockets in my patients because I firmly adhere to this technique.
Even though the correct implant size is selected, and the pocket is created correctly, why do implants still occasionally move to the sides when lying down? The answer is “tissue stretch.” If the outer breast border is set correctly, excessive tissue stretch laterally (towards the outer chest wall) can create more room for the implant as the breast tissue thins in response to stretching, losing its ability to contain the breast more centrally on the chest when lying down. When upright, the implant does not move towards the outer chest but when lying down, gravity causes the implant to fall along the curved chest wall towards the side of the chest. For example, if you place a 300 cc implant into the breast with a snug fit, we can assume the pocket size to be approximately 300 cc. However, over time, due to gravity, possibly thin, poor quality tissue (and sometimes even with good tissue), the breast tissue will stretch. Think of the breast as a bag containing an implant. As the breast stretches, the pocket volume will increase. Now the implant is much smaller relative to the breast pocket volume. When standing, the breasts look pretty good because the lower crease is holding the implants in the proper position. However, when lying down, the lower breast crease has no effect on implant position and the implants slide along the lateral curvature of the chest wall and fall to the sides, sometimes leaving a contour deformity on the middle of the chest because now the breasts are relatively under filled.
A brief word about tissue stretch. Whenever a breast implant is inserted into the breast, the breast tissues will stretch. The degree that the breast will stretch is not predictable. The two main factors that will increase tissue stretch are: poor quality tissue to begin with (thin, poor elasticity, sagging), and placing a particular sized implant in the breast where the implant size exceeds the ideal breast volume as determined by precise preoperative measurements and planning as I do for all my breast augmentation patients. Certainly, the patients who have the best quality tissue and do not exceed the size implant as recommended by my preoperative measurements will stand the best chance of having the least amount of tissue stretch following augmentation surgery. However, there is one other factor that will lead to an increased, undesirable degree of tissue stretch and that is genetic predisposition, an entirely unpredictable factor. I have seen patients with poor tissue not stretch much after surgery and I have seen patients with excellent quality tissue overstretch considerably.
In some cases, the problem can even be a combination of these two factors. In most cases, the problem of the implant moving too far to the side is due to excessive tissue stretch rather than errors in the creation of the implant pocket. The more compromised the breast tissue, the greater the likelihood that this problem will occur.
How I Assess a Breast for Lateral Displacement/Lateral Implant Malposition
When I assess a breast for this problem, there are two things to consider:
- Does the breast implant shift too far laterally when the patient is lying upon her back?
- Is the lateral breast crease in the proper location or is it too far to the side?
When I create the implant pocket at surgery, I set the lateral breast crease at the very outer edge of the breast. This usually falls at approximately the mid-lateral line of the chest.
Isolated Lateral Displacement
Isolated lateral displacement refers to stretching of the lateral or outer breast tissue alone. Therefore, I am referring to the distance from nipple to the lateral or outer breast crease. As long as the outer breast crease lies in the correct place, then the breast pocket was created properly. What has happened is that the breast tissue has stretched more than desired, causing the implant to re-distribute its volume into the outer breast, much in the same way as was the case on the lower breast where there is lower pole stretching.
Lateral Implant Malposition
This situation is analogous to that of inferior implant malposition. Rather than the implant redistributing its volume laterally, the entire implant is shifted laterally. The end result is that the breast outer edge appears too far laterally on the chest wall. This is important to know if one is contemplating surgical correction. It is imperative to understand the anatomy and the cause of a deformity in order to formulate a corrective surgical plan. The surgeon needs to understand if the problem is due to stretching of the lateral portion of the breast, over dissection of the lateral breast crease or a combination of the two. This will allow the surgeon the best opportunity to formulate the most optimal surgical plan for correction of the deformity.
The below diagram illustrates the difference between Isolated Lateral Displacement and Lateral Implant Malposition.
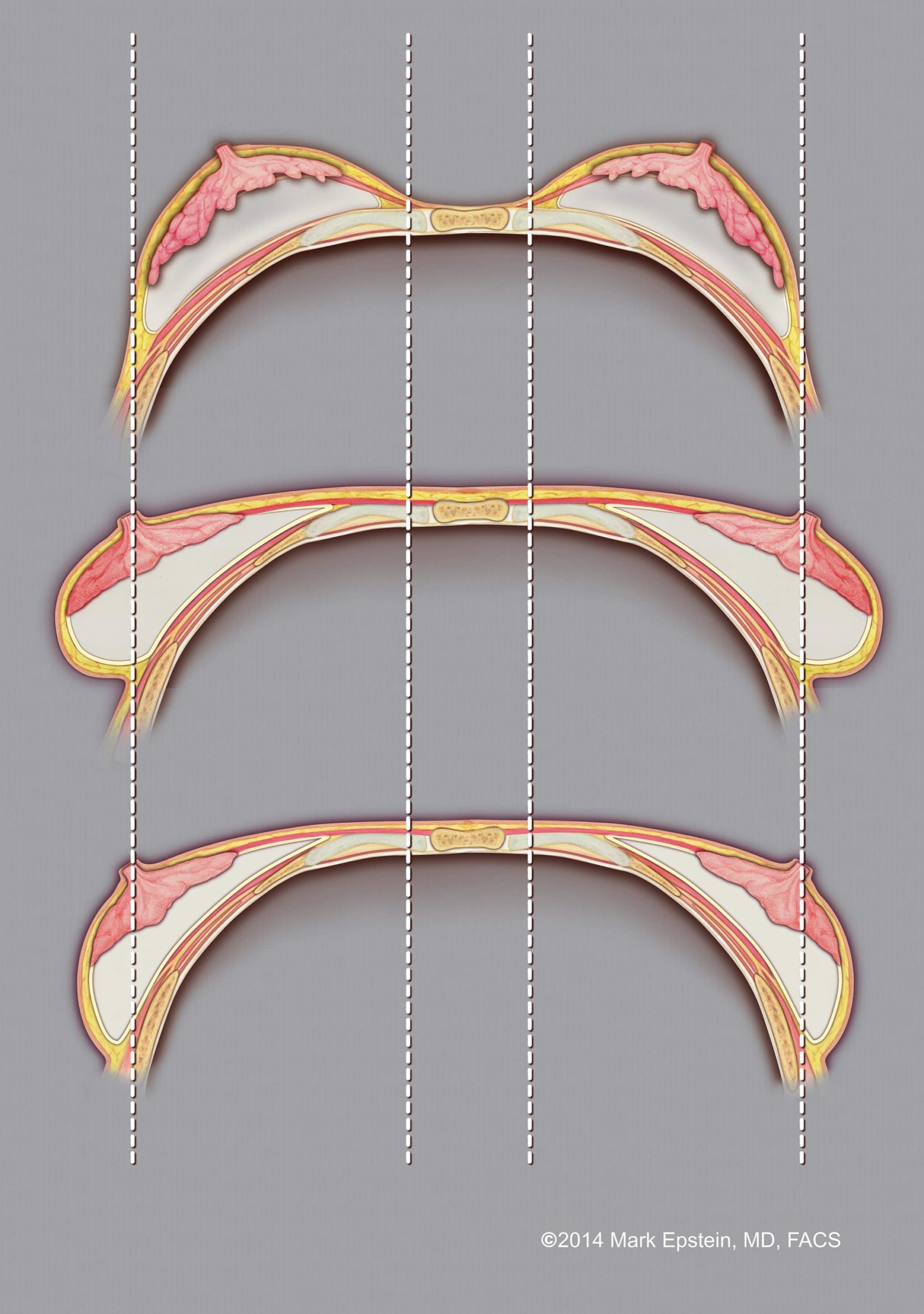
Top: Breast implants sitting atop the chest wall, with no lateral displacement or malposition. The vertical lines show the inner (medial) and outer (lateral) borders of the implant pocket.
Middle: Isolated lateral displacement. The outer border of the implant pocket is in alignment with that of the top figure, however, the outer aspect of the breast itself has stretched, resulting in some of the breast volume shifting laterally. In this case, the outer pocket border was set in the correct place, however, it is due to isolated tissue stretch of the breast tissue alone that results in the breast implants moving to the side.
Bottom: Lateral implant malposition. The outer border of the breast pocket lies further laterally than in the top two figures. In this case, the pocket was opened too far to the side, resulting in the implant itself shifting laterally as well.
In either the case of isolated lateral displacement or lateral implant malposition, there is a shift in breast implant volume to the sides, leaving the inner breast deficient in volume when lying in the supine (on your back) position, creating a volume void near the breastbone. Either situation can result in a cause for concern on the part of the patient. When I am in consultation with a patient whose breast skin has very poor elasticity, I counsel them that several months after surgery, she may develop lateral breast stretching resulting in isolated lateral displacement of her breasts when lying upon her back.
Prev Topic: Correction of Lower Pole Stretch / Inferior Implant Malposition »
Next Topic: Correction of Lateral Displacement / Lateral Implant Malposition »
Sections – Implant malposition/bottoming out of the breast
- Incorrect Development of the Pocket
- Correction of Incorrect Development of the Pocket
- Lower Pole Stretch / Inferior Implant Malposition
- Correction of Lower Pole Stretch / Inferior Implant Malposition
- Lateral Displacement / Lateral Implant Malposition
- Correction of Lateral Displacement / Lateral Implant Malposition
- Synmastia / Medial Malposition
- Correction of Synmastia / Medial Malposition
Prev Section: Explantation (Removal of implants) »
Next Section: Change of Implant Size »
Sections – Revision of Breast Augmentation
- Capsule contracture
- Explantation (Removal of implants)
- Implant malposition/bottoming out of the breast
- Bio-materials Used in Revision of Breast Augmentation – Strattice, GalaFLEX and GalaFORM
- Implant size change
- Change from textured to smooth implants
- Changing from saline to silicone gel filled implants
- Adding a breast lift later
Prev Chapter: Important Things to Consider When You Decide to Move Forward With Breast Augmentation »
Next Chapter: ALCL and Breast Implant Illness »
Chapters – Breast Augmentation Guide
- Intro to Breast Augmentation
- Preservation Breast Augmentation – A New Era!
- Motiva Implants – What You Need to Know
- Five key decisions you need to make
- One-Day Recovery Breast Augmentation
- Anesthesia – General, Sedation or Local?
- Breast Lift (Mastopexy) with/without Implants or Fat
- What else should I know about breast augmentation?
- Important Things to Consider When You Decide to Move Forward With Breast Augmentation
- Revision of breast augmentation
- ALCL and Breast Implant Illness
Schedule A Consultation
Contact our Long Island office at 631.689.1100 for more information regarding repair of implant malposition.
