
Part I: Understanding the Anatomy
The best way to understand "above or below the muscle" is to first understand the relevant anatomy. It is not difficult to understand and will help you greatly to understand the different surgical planes that a breast implant can be placed. By surgical plane, I am referring to a space that is created during surgery when two layers of tissue that normally lie one on top of the other are now separated, creating a space.
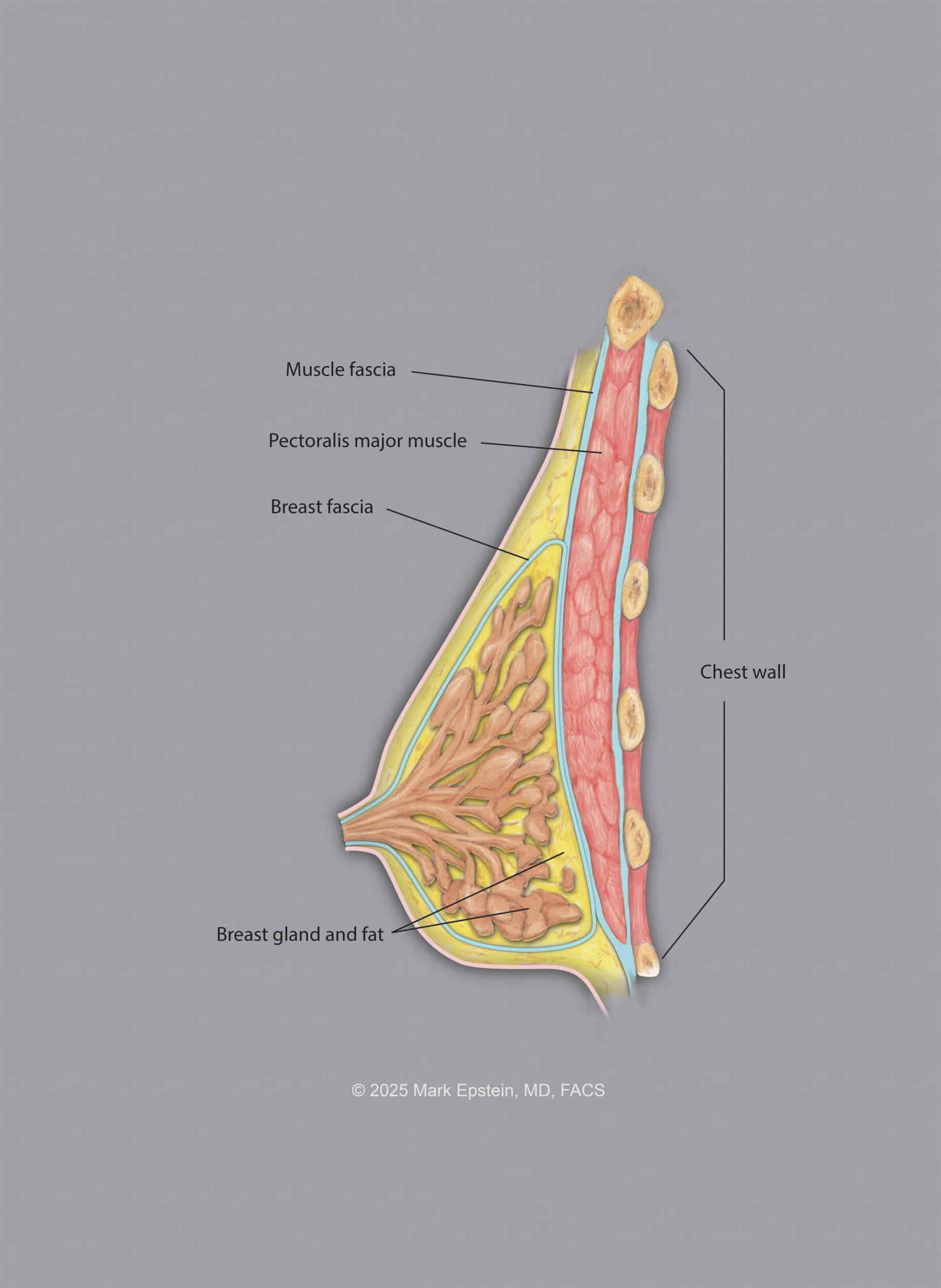
Anatomy of the breast: the breast is comprised of fatty and glandular tissue. This is surrounded by a thin layer called a capsule or fascia. There are ligaments that run vertically through the breast called Cooper's ligaments.
There is also a circular ligament that surrounds the periphery of the breast called the Circummammary ligament. You can think of it like a "gasket" that lies in a circle on the chest wall, acting as a "ring of attachment" that affixes the breast to the chest wall. This is shown below:
The Circumammary Ligament
The breast glandular tissue and fat with its surrounding fascia lies on top of another thin layer of tissue called the pectoralis fascia. This fascia in turn lies on top of the pectoralis major muscle (the "pecs"), which lies on top of the chest wall (rib cage and rib muscles).
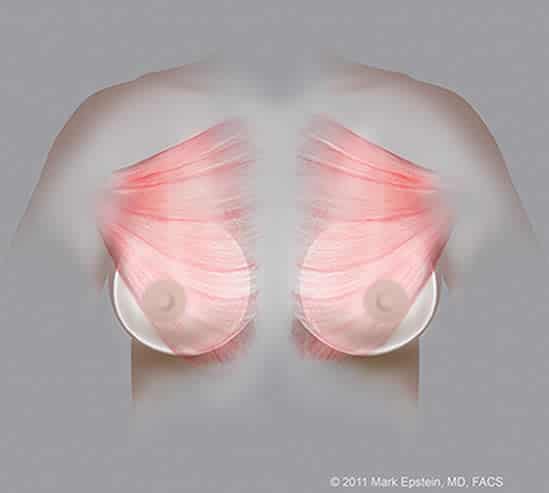
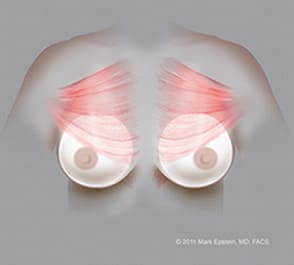
The pectoralis muscle is a triangular shaped muscle that has a broad attachment along the sternum (breast bone) and the medial (inner) side of the ribs near the sternum, then spans across the chest to attach on the humerus (upper arm bone). There are actually several "planes" in which to place the implant. These are described below.
Below the Muscle
Submuscular Plane (Dual Plane)
Submuscular - Between the chest wall below and the pectoralis muscle above. In reality, the muscle only covers the upper 60-80% of the implant because the muscle is not large enough to cover all of the implant. You also do not want to have total submuscular coverage - it looks very freaky and fake - like a ball on the chest wall. The rest of the implant (the bottom and lower, outer portion) lies under the breast itself. This is the only plane that is under the muscle; all of the following planes lie above the pectoralis muscle.
When you cut the muscle, it retracts upwards leaving the lower portion of the implant covered by only muscle. That is why it is called "Dual Plane" - because the upper part of the implant is covered by muscle and the lower part is covered by breast tissue only. By selectively releasing the muscle from below, the degree of upwards retraction of the muscle can be varied and controlled. Additional release of the muscle so that the lower edge of the muscle is at the level of the nipple is called a Dual Plane II, and a release to the level of the upper areola is called a Dual Plane III. No additional release at all is a Dual Plane I.
This is shown below.
Above the Muscle
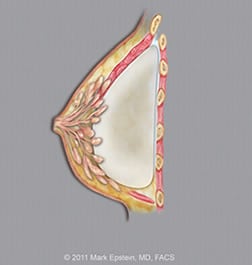
Subfascial Plane
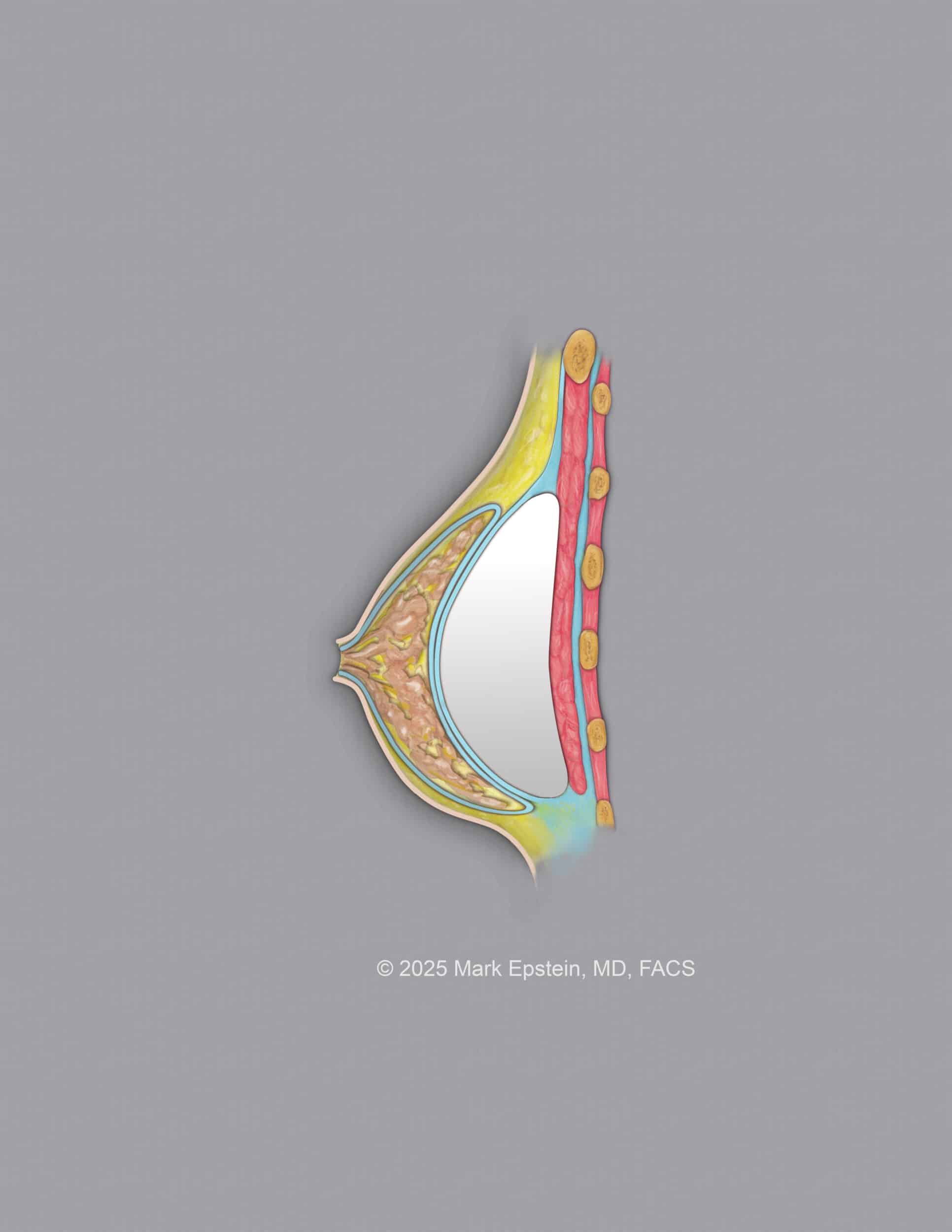
Subfascial - Between the pectoralis muscle below and the pectoralis muscle fascia above. The fascia is a very thin layer of tissue, but there is some clinical evidence to suggest that placing the implant in this plane is superior to placing the implant above this plane, possibly because of the maintenance of attachments of Cooper's ligaments in the breast to the fascia. This is shown below.
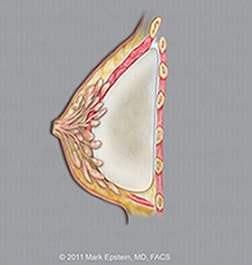
Subglandular Plane
Subglandular - Between the pectoralis muscle fascia below and the capsule of the breast gland above. This is a less tedious dissection for the surgeon than the subfascial plane. Clinical results are reported as better for subfascial than for subglandular placement. The subglandular plane is shown below.
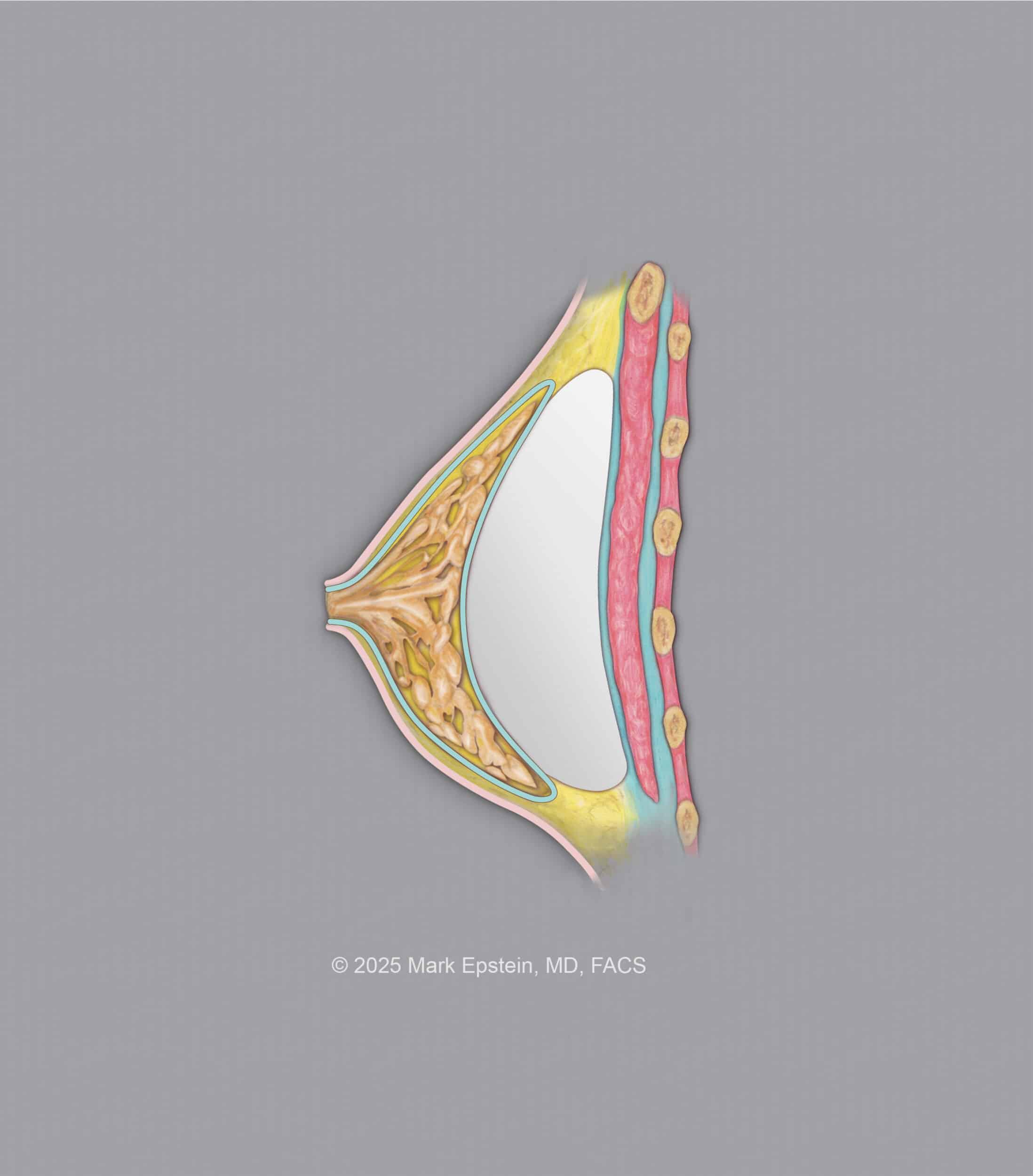
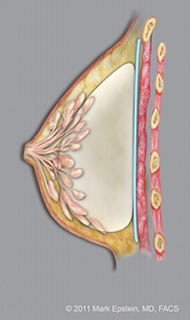
Breast Preservation Space
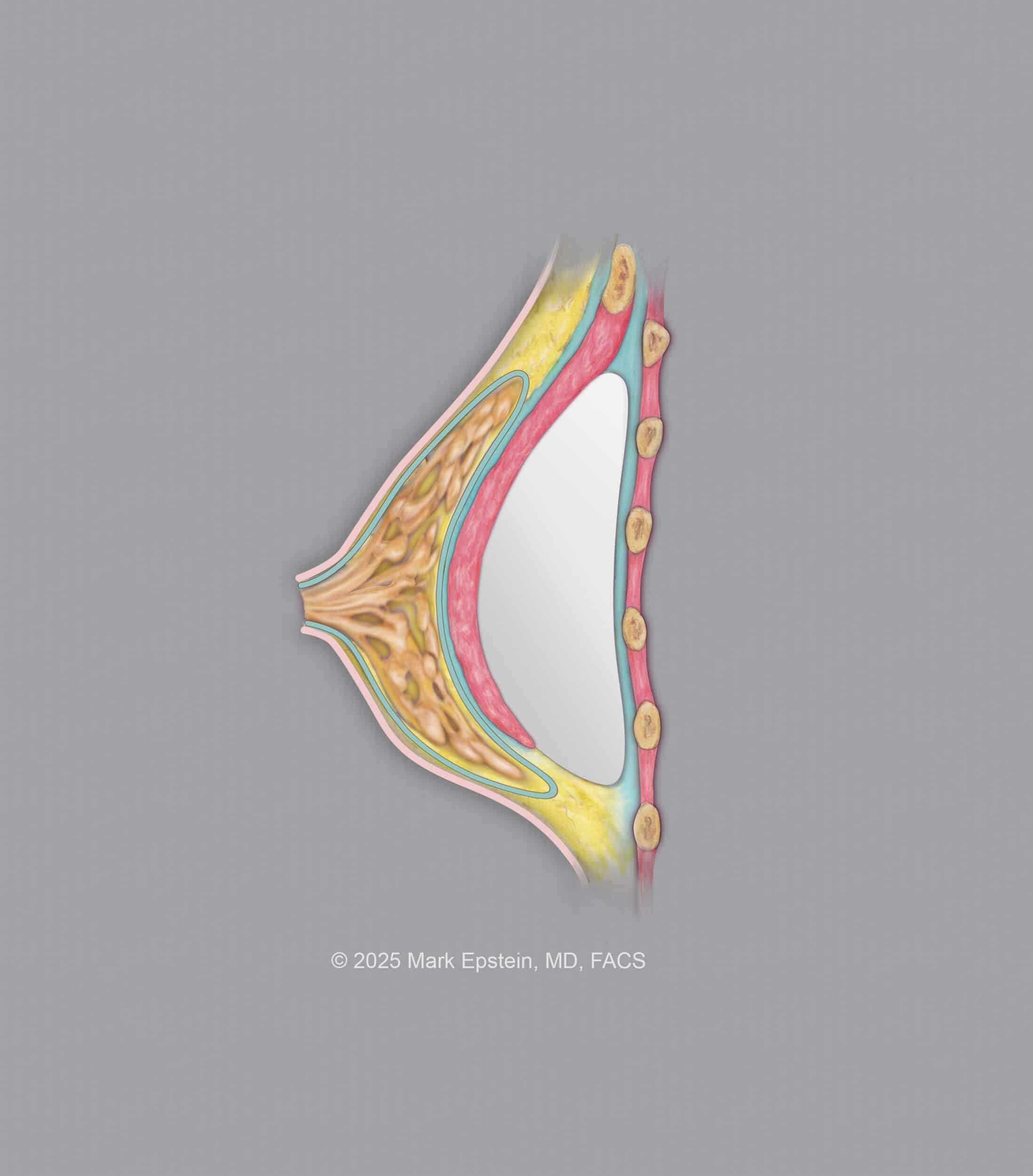
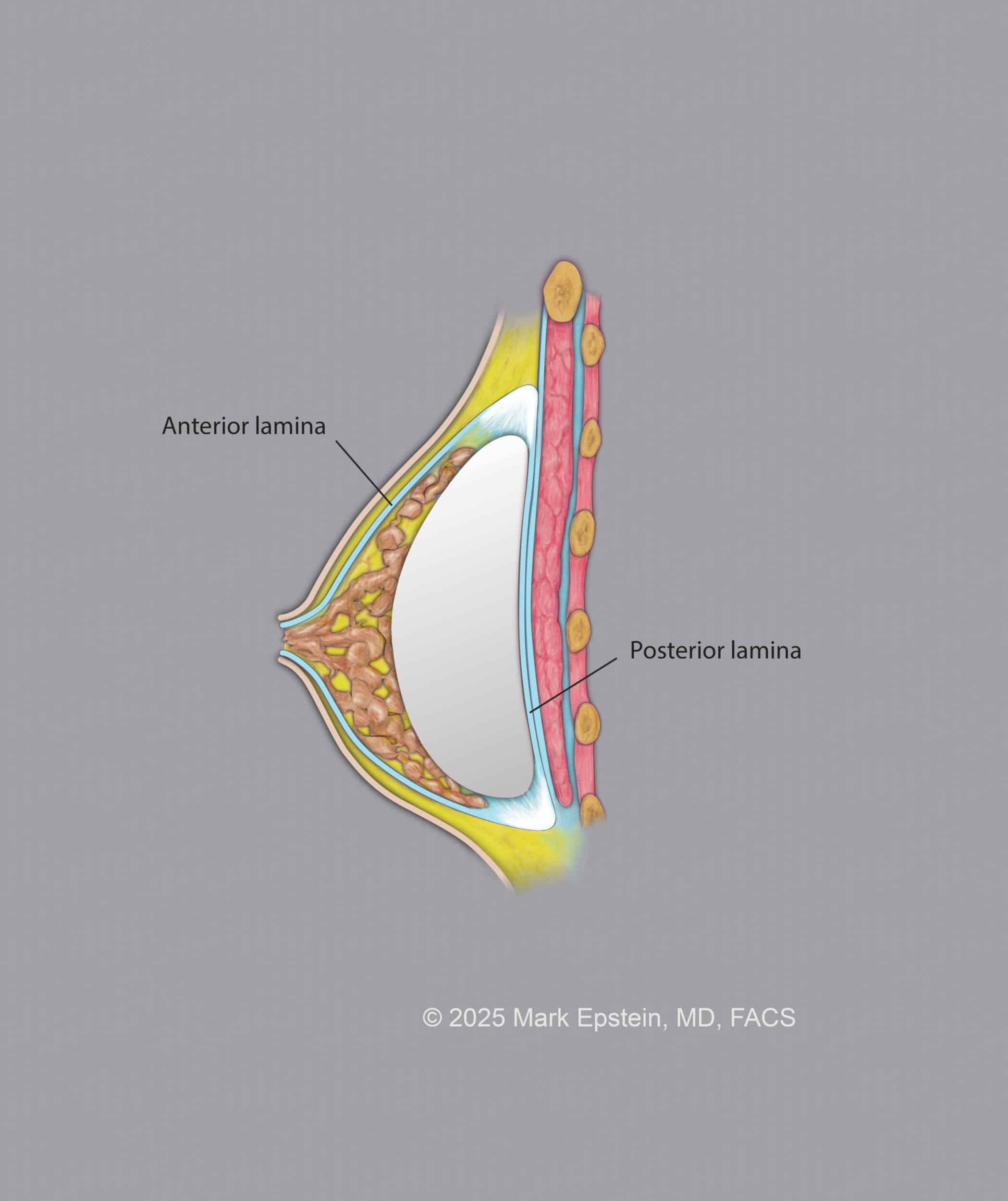
Preservation plane - Between the capsule of the breast below and inside the breast itself. This is a relatively new concept. The advantage of this plane is the maintenance of all the ligaments in the breast, as well as the circumammary ligament which encircles the breast and attaches the breast, like a gasket, to the chest wall. The surgical approach for the other planes disrupt this ligament, but it is preserved when placing an implant into this plane, hence the name "Preservation Space." Special equipment is required for this procedure. The anterior lamina and posterior lamina are the fascia that envelopes the breast glandular and fatty tissue.
When an implant is in the "Preservation Space", it likes between the posterior lamina (layer) of the breast and the "corpus mammi", also known as the breast gland and fat.
This is shown below.
Part II: Advantages and Disadvantages of Each Plane
Submuscular Plane (Dual Plane)
Advantages:
Easy dissection. Using very gentle techniques of dissection, there is no more discomfort than with a prepectoral (above the muscle) pocket. Note that the muscle does not completely cover the implant, which is covered only by the breast in the lower, lateral quadrant.
For those with a type II sagging breast (mild to moderate), a dual plane II or III approach will correct the bottoming out (see below case example showing the power of the dual plane technique). The dual plane technique involves repositioning the lower portion of the pectoralis muscle upward (see diagram below) so as to allow the implant to better fill out the lower portion of the breast and allow the nipple to rotate upward into a more favorable position. As the nipple is in proper position, no breast lift is required. It is also important to note that when there is more severe sagging and the nipple position is too low, a formal breast lift may still be required.
Up until 2025, I believed that with the advent of the dual plane approach, there is absolutely no indication to ever perform a prepectoral (above the muscle) augmentation. I could not be any more wrong!!! With the FDA approval of the Motiva breast implant, I have now changed my opinion on this.
- Disadvantages: Most would say that there are four main disadvantages:
- The first is recovery time, many believe that placing the implant above the muscle is less painful and leads to a shorter recovery. Contrary to popular belief, if surgical dissection is performed in a minimally traumatic manner, as with the "One-Day Recovery Breast Augmentation Technique", recovery time and discomfort are no worse that with any a subfascial or subglandular approach. The Breast Preservation Plane has the fastest recovery of all.
- When placing an implant below the muscle, there is a potential for an "animation deformity", that is, when the muscle contracts, the breast deforms as the implants are moved apart from each other. It then reverts entirely to normal when the muscle ceases to contract.
- Cleavage: Everyone wants cleavage. You cannot move the position of the breast on the chest wall. However, it is important to understand that when placing the implant below the muscle, the muscle acts as a barrier to medial position of the implant. If the implant is placed above the muscle, then it can be positioned a little closer to the midline of the chest.
- The last is called a "waterfall deformity." Implants do not lift the breast. When there is a fair amount of native breast tissue in front of the implant, which is sitting atop the muscle, with time, that breast tissue will slide off and descend from the muscle, leading to an abnormal distribution of breast tissue on the lower breast, and in some cases, with the nipple lower as well. This is seen in cases of weight loss with compromise of the breast tissue quality, post pregnancy/lactation, or with weight gain where the native breast tissue volume increases.
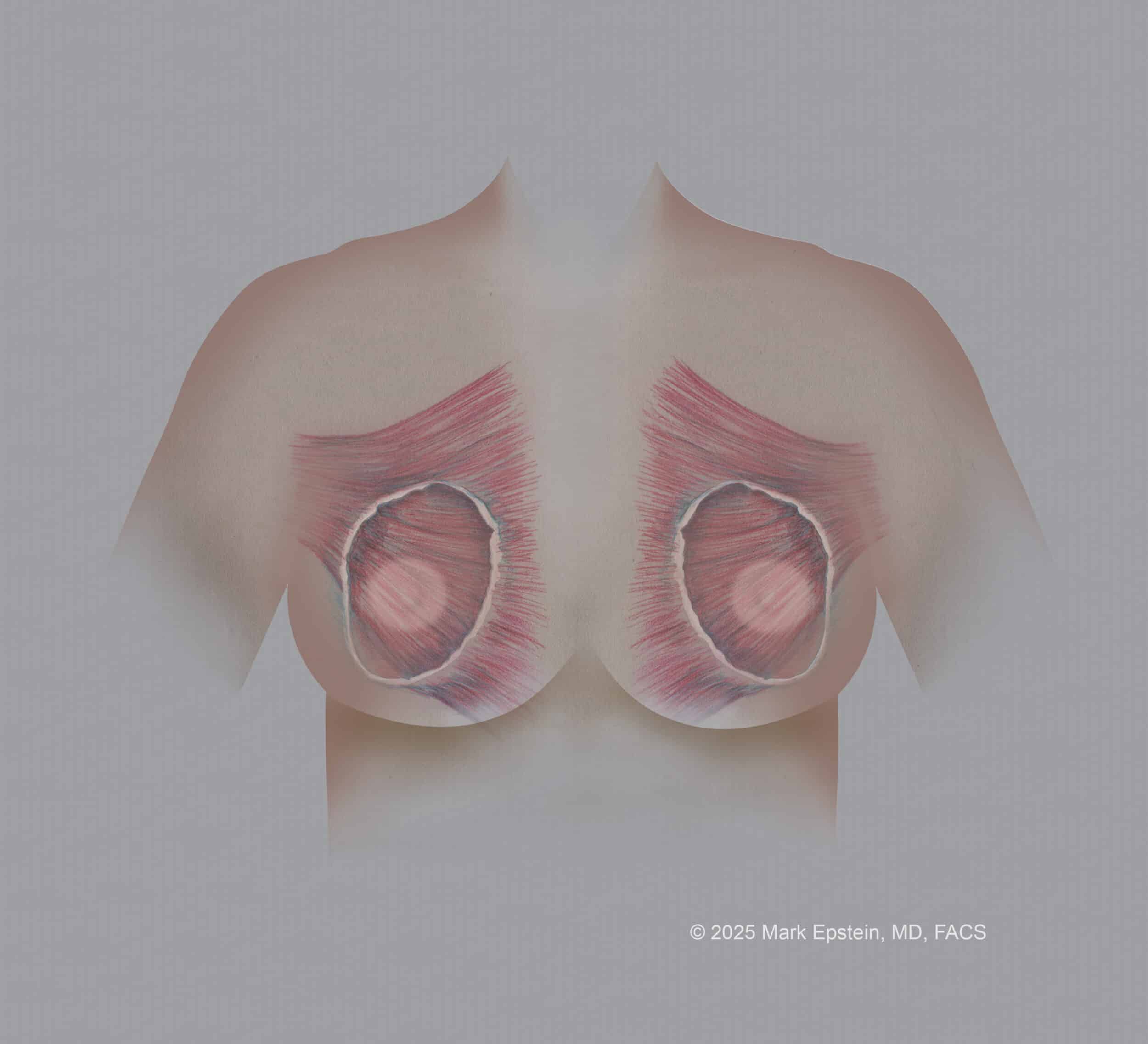
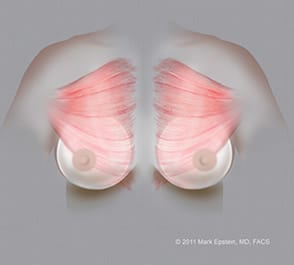
The difference between placing the implant above the pectoralis muscle versus below the muscle (front view):
Click on an illustration below for a larger version:
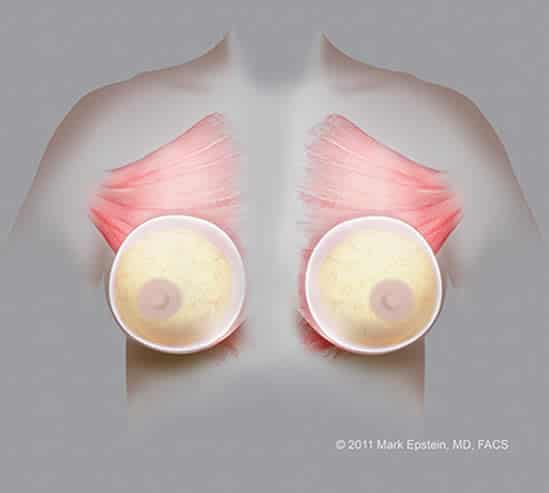
Subglandular implants – AP ©2011 Mark Epstein, MD, FACS
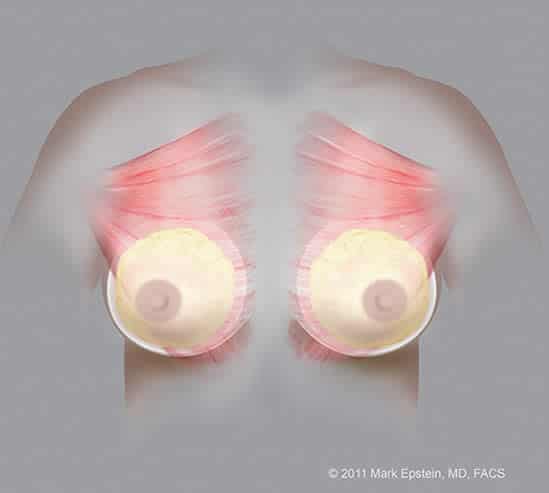
Partial Retropectoral Submuscular implants (with breast gland shown) – AP ©2011 Mark Epstein, MD, FACS
Partial Retropectoral Submuscular implants (with breast gland removed from drawing) – AP ©2011 Mark Epstein, MD, FACS
The difference between placing the implant above the pectoralis muscle versus below the muscle (side view):
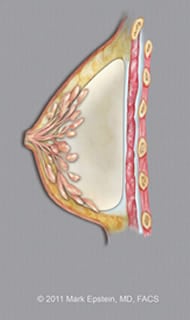
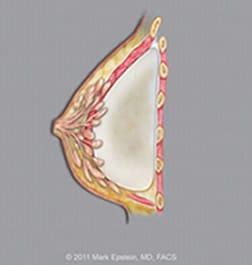
Subglandular implants – LAT ©2011 Mark Epstein, MD, FACS

Retropectoral Submuscular implants – LAT ©2011 Mark Epstein, MD, FACS
Dual-Plane I, II and III
The technique of dual-plane augmentation, originally described by John Tebbetts, M.D. This technique involves the creation of a pocket below the pectoralis major muscle in which the implant will be placed. A second, smaller pocket is created between the muscle and the above glandular tissue, usually up to about the level of the nipple or upper border of the areola (the pigmented skin around the nipple). Nothing is placed in this pocket, but the separation of tissues serves to separate the tighter muscle with the overlying stretched breast tissue to permit the implant to better fill out the lower pole of the breast, thus preventing the "double-bubble" deformity as described above. This technique leverages the advantages of both a subpectoral approach (pleasing upper beast contour where it takes off from the chest wall) with that of a subglandular technique (pleasing lower breast contours). The dual plane technique adds additional time to the procedure, but can make all the difference in obtaining a beautiful, natural augmentation as opposed to a poor, unnatural look, with breast tissue sliding downward over the front of the breast. This has been the workhorse of my practice for about thirty years, and I have attained wonderful results with dual plane submuscular placement of breast implants.

Submuscular implants (Dual plane I) – AP ©2011 Mark Epstein, MD, FACS
Submuscular implants(Dual plane I) – LAT ©2011 Mark Epstein, MD, FACS
Submuscular implants (Dual plane II) – AP ©2011 Mark Epstein, MD, FACS
Submuscular implants Dual plane II) – LAT ©2011 Mark Epstein, MD, FACS
Submuscular implants (Dual plane III) – AP ©2011 Mark Epstein, MD, FACS
Submuscular implants (Dual plane III) – LAT ©2011 Mark Epstein, MD, FACS
The dual plane III placement seen below allows the implant to better fill out the lower portion of the breast by re-positioning the lower edge of the muscle upward (note less muscle coverage of the implant in the area of the nipple as compared to the partial retropectoral Dual Plane I and II placement, 2 diagrams above, on the right).
Secret tidbit - When the lower edge of the pectoralis muscle is elevated off the chest wall to gain access to the space below the muscle, the muscle naturally retracts upwards for a few cm. This is what Dr. Tebbetts termed a Dual Plane I. So, when you place an implant below the muscle, the lower portion of the implant is actually covered only by breast tissue. This is why, especially with saline implants, the implant is often palpable in the lower portion of the breast. A dual plane II or III is an extension of this concept.
The best way I can explain what a dual plane procedure is: In a sub-muscular pocket, the lower portion of the breast is below the lower edge of the pectoralis muscle, so the majority, but not all of the implant is covered by muscle; perhaps the upper 80% is covered by muscle and the lower 20% by breast tissue only. (If you had 100% muscle coverage of the implant, it would look very unnatural, firm and spherical.) We call this a "Dual Plane I." So, technically speaking, a sub-muscular (or as it is otherwise known as a partial retropectoral) pocket is really a combination of above and below the muscle, whereas the traditional subglandular pocket is exclusively above the muscle. Now, if you imaging the lower edge of the pectoralis muscle sliding upward and providing, perhaps, coverage of the upper 65% of the implant with muscle and 35% (these numbers are for illustration purposes only) of the implant with breast tissue only, then you have a Dual Plane II pocket. Now, slide the muscle up a little further so that there is muscular coverage of the upper 50% of the implant with muscle and 50% coverage of the implant below with breast tissue only, now you have a Dual Plane III.
With the approval of the new Motiva implants, I have changed what I advocated for the past 30+ years and now for primary (first time breast augmentation with/without a lift) my choice is either subfascial if I am doing a "typical breast augmentation" (not Preserve - Preservation Augmentation), and the Preservation space if I am doing a Preserve breast augmentation. The results are simply better and more natural in my opinion, with better cleavage and without the animation deformity of the below muscle approaches.
Above the Muscle Placement
When placing an implant above the muscle, there is the choice of the Subglandular, Subfascial and Preservation planes. As a whole, there are certain advantages and disadvantages to placing the implant above the muscle in general, and with each of those three planes, there are again advantages and disadvantages.
- Advantages:
Easy dissection. There is a myth that there is less associated pain than placement under the muscle, but in my opinion and experience with the 24 hour recovery technique, this is not true.
The cosmetic appearance of the breast, in my opinion, is more natural when the implant is above the muscle.
It is easier to achieve a more desirable cleavage, as the implants are not being held apart from the midline by the muscle where it attaches to the breast bone.
There is no "animation deformity" - which is when the pectoralis muscle contracts, the breasts move and indent.
There is no "waterfall deformity" which is where the implant stays high, but with time the breast tissue and nipple slowly roll off the implant producing a "Snoopy dog nose" like contour.
- Disadvantages:
Without muscle overlying the upper portion of the implant, there is less tissue above the implant to pad it so that rippling and wrinkling may be more obvious, and the implant may be more visible and palpable. This is a decision that needs to be made considering the quality and the amount of available breast tissue. In the past, I recommended to patients that they have at least 2 cm thickness of tissue in the upper breast to prevent these issues. Now, with the Motiva breast implants, which are the only generation six breast implants available today, are better suited to placement above the muscle, requiring only about 1 cm of tissue thickness in the upper breast. If there is a still a concern about needing some extra tissue thickness in the upper or inner breast (cleavage), this can be easily resolved with fat transfer.
Some breast radiologists believe that this approach interferes with mammographic visualization of the breast. In some cases, the breast tissue at the periphery of the breast may be a little more difficult to image and require additional mammographic views. The reality is that when placing implants below the muscle, as the muscle only covers the upper 1/3 to 2/3 of the breast, the same issue occurs at the lower breast anyway. The truth is, with multimodality breast imaging (mammogram, ultrasound, MRI) the entire breast can be safely and adequately imaged to screen for breast cancer.
The Motiva implant has become a gamechanger in my practice. As a clinical investigator in the US FDA MOTIVA Clinical Trial, I have performed numerous breast augmentations with the Motiva implant in the submuscular position. That said, I am with rare exception placing the Motiva implants above the muscle in primary augmentations! I think that the breasts look more natural than they ever have and my patients absolutely love them. They feel like natural breast tissue, even when placed above the muscle!
Subglandular Placement
- Advantages: Easiest dissection. The implant is placed above the muscle fascia, so this does not need to be dissected from the muscle below.
- Disadvantages: Many surgeons believe that keeping the fascia intact with the breast preserves the overlying Cooper's ligaments. When an implant is placed in this plane, the attachment of the muscle fascia to the overlying breast gland is cut.
Subfascial
Some surgeons talk about a subfascial pocket. The only difference between this and a subglandular pocket is that the thin (1 mm or less) tissue covering the front surface of the pectoralis major muscle, the "pectoralis fascia", is elevated off the muscle and left attached to the underside of the breast tissue. In my opinion, and that of others, preserving this thin, gossamer layer of tissue seems to result in a superior appearance to the breast.

Subfascial implants (with implant shown under the muscle fascia shown as a blue line) – LAT ©2011 Mark Epstein, MD, FACS
Subglandular implants (with implant shown over the muscle fascia shown as a blue line) – LAT ©2011 Mark Epstein, MD, FACS
How powerful is the dual plane technique? In the example below, if the dual plane technique was not used, the breast tissue would hang off the front of the implant and create a “snoopy dog deformity” as viewed from the side.
Pre-Op



Post-Op



So which is better: “above the muscle” or “below the muscle”?
When the implant is placed below the muscle, there is more soft tissue coverage of the implant, which gives the implant more support and makes it less palpable. With generation 5 implants (Allergan Natrelle, Mentor and Sientra), in my opinion, the upper portion of the breast may look better when the implant is below the muscle.
The new generation six Motiva implants are much more suited to placement above the muscle. There is a more natural feel and appearance to the breast, with better opportunity to attain a narrower cleavage, no animation deformity and minimal chance of waterfall deformity.
When having mammography performed, the mammographer will use techniques such as the Eklund breast displacement technique to better image an augmented breast regardless of whether the implant sits below or above the muscle.
I do not believe that there is a significant difference in capsule contracture of the breast with either implant placement.
The fact is that on the lower and lateral portions of the breast, there is rarely muscle coverage of the implant, and thus the difference between below and above the muscle placement of the implant does not even apply to this area of the breast.
What if my breasts are sagging? Should the implant be above or below the muscle?
Ptosis means drooping or sagging of the breast. There are two types of ptosis, and they can co-exist in the same breast. The treatment for each type, however, is very different. Women with no (true) ptosis (drooping of the nipple) or pseudoptosis ("false ptosis" or bottoming out of the breast tissue with loss of superior fullness and a drooping bottom contour to the breast), are candidates for either above the muscle (subglandular) or below the muscle (subpectoral) placement of the implant, assuming that they have good quality tissue to drape over the implant.
Women with pseudoptosis present a more challenging problem. Pseudoptosis is more common in women who have been pregnant, and often more pronounced in women who have breastfed their children. In pseudoptosis, the nipple may or may not be at appropriate height (at or above the level of the lower breast crease or inframammary fold). The loss of superior fullness of the breast with shifting of the glandular and fat tissue of the breast to the lower portion of the breast (drooping of the lower portion of the breast as manifested by a longer distance from the crease below the breast to the nipple) is more problematic if one wishes to place the implant below the muscle. In this case, implant placement below the muscle would result in a "snoopy-dog deformity". The muscle with the underlying implant will project forward; however, the glandular breast tissue will "fall" off the front of the implant ("waterfall deformity"), leading to the appearance of a nice breast mound with a sagging wad of breast tissue at the bottom. It is in these cases that surgeons usually elect to place the implants above the muscle. This better fills out the lower breast tissue, and lets the implant descend a little more within the breast envelope to yield a more natural look. In cases where the breast is very stretched out, the envelope size of the breast (the potential space for the implant) tends to be larger, and requires a larger implant to fill the breast out. While that may make a lot of women happy at least initially, a larger, heavier implant supported by a stretched out, poor quality soft tissue envelope will often times lead to over-stretching of the breast and further descent of the implant. In these cases a simultaneous breast lift to reduce the size of the skin envelope of the breast and lift the nipple may be prudent.
Here is my opinion, based upon a great deal of experience:
Good quality tissue, minimal sagging - Above the muscle
Good quality tissue, moderate or worse sagging
- Traditional Augmentation above the muscle with a lift and soft tissue support (GalaFlex)
- Preserve Augmentation above the muscle with a lift. There is no need for soft tissue support due to the preservation of the breast ligaments with this procedure.
Very compromised tissue, with or without sagging
- A below the muscle approach MAY be indicated, with or without a lift.
- Above the muscle approach probably preferred, using Preserve technique to preserve the ligamentous support of the breast
A thorough examination and assessment of the breast tissues is required so as a proper surgical plan can be made. One cannot use this website as a tool to decide what technique is indicated. This is a complicated subject, requires a great deal of surgical knowledge and experience and decision should be made by a person possessing this extent of knowledge and experience.
Determining whether a dual plane below the muscle approach is sufficient or if a lift is required as well is discussed in greater depth in the chapter Will I need a breast lift (Mastopexy)?.
How does a Dual-plane technique fit in?
The practice of surgery, and medicine in general, should be very fluid. A surgeon needs to be able to pivot and change their practice and beliefs based upon the most current information and technology. Such has been the way I have practiced medicine and surgery over the past forty or so years. Whle for decades, I believed strongly in placing implants below the muscle, with the advent of newer technology in implant placement techniques and the new generation six Motiva implants, I am achieving superior results using implant placement above the muscle.
ALthough my preference now is above the muscle, if a patient specifically requested her implants to be placed below the muscle, would I perform the surgery - absolutely! I offer options and each patient needs to take the path that best suits their desires and goals.
Prev Section: What size implant should I get? »
Next Section: Incision location? »
Sections – Five Key Decisions You Need To Make
Chapters – Breast Augmentation Guide
- Intro to Breast Augmentation
- Preservation Breast Augmentation – A New Era!
- Motiva Implants – What You Need to Know
- Five key decisions you need to make
- One-Day Recovery Breast Augmentation
- Anesthesia – General, Sedation or Local?
- Breast Lift (Mastopexy) with/without Implants or Fat
- What else should I know about breast augmentation?
- Important Things to Consider When You Decide to Move Forward With Breast Augmentation
- Revision of breast augmentation
- ALCL and Breast Implant Illness
